What Makes Silent Reflux Different from Ordinary Heartburn?
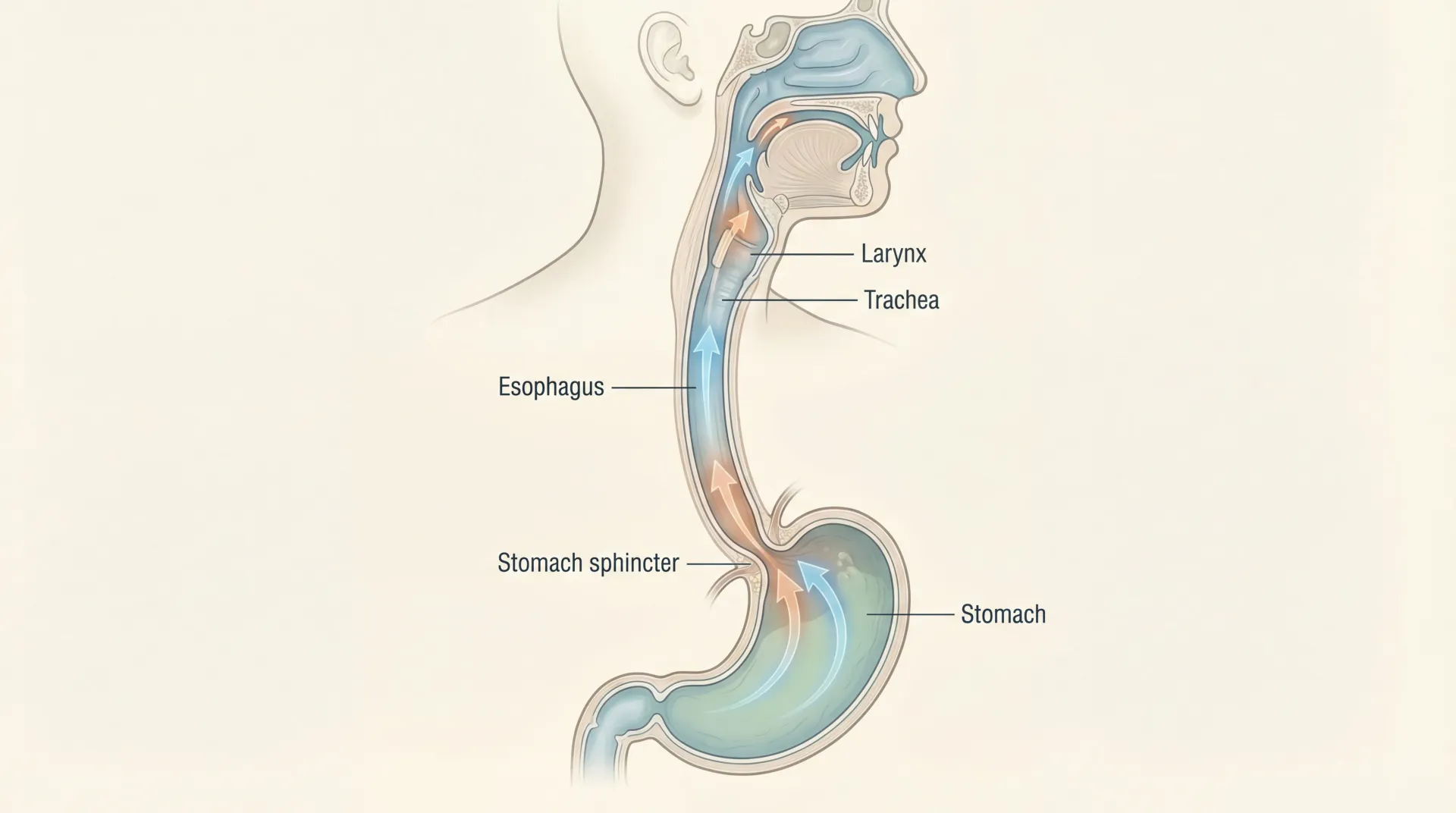
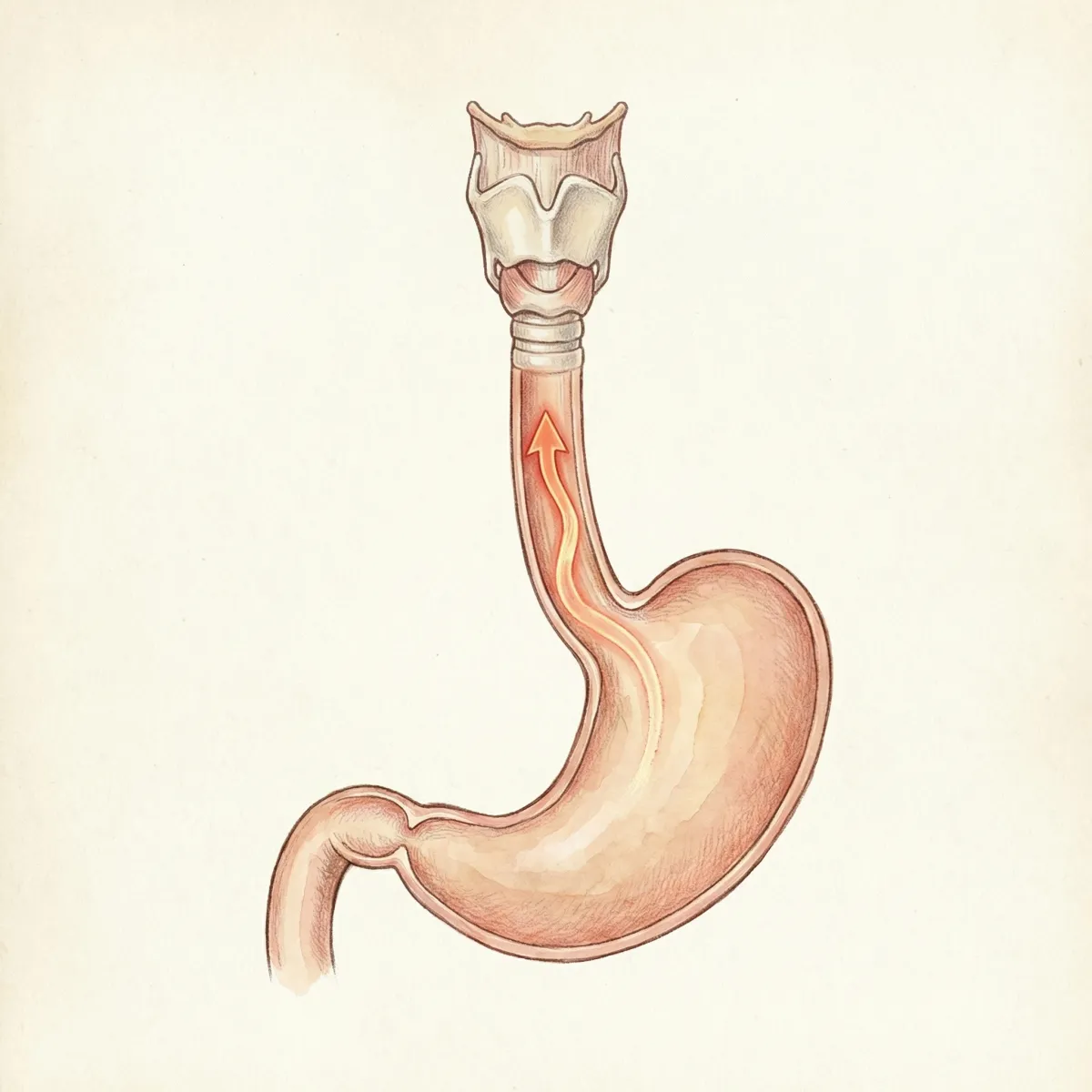
Silent acid reflux, usually called laryngopharyngeal reflux or LPR, happens when stomach contents move upward into the throat, voice box, and upper airway tissues. Unlike classic reflux, many people do not report regular burning in the chest. That absence of obvious heartburn is why this condition is often missed for months or even years. The underlying biology still involves refluxate, but the tissue being exposed is different and the symptom pattern is different.
Population-level digestive disease guidance from the U.S. National Institute of Diabetes and Digestive and Kidney Diseases explains that reflux symptoms vary widely and can include extra-esophageal symptoms. Clinical guidance from the American College of Gastroenterology guideline also notes that symptoms outside the chest are common, but diagnosis requires careful interpretation because throat symptoms are not specific to reflux alone.
One practical way to think about LPR is this: GERD is often symptom-heavy in the chest, while LPR is often symptom-heavy in the throat and voice. Many patients have overlap, but not everyone does. That distinction matters because treatment decisions should be made using the symptom cluster plus objective testing when available, not by one symptom alone.
| Feature | LPR (Silent Reflux) | Classic GERD Pattern |
|---|---|---|
| Most common complaint | Throat clearing, hoarseness, globus, chronic cough | Heartburn, regurgitation |
| Typical location of irritation | Larynx, pharynx, upper airway | Lower esophagus |
| Nighttime relevance | Often worse when supine and after late meals | Often worsens after large meals and lying flat |
| Diagnostic challenge | High, because symptoms overlap with allergy, infection, voice strain | Moderate, with stronger symptom specificity |
Quick clinical takeaway: no heartburn does not rule out reflux-related injury in the throat. Persistent hoarseness, chronic throat clearing, and cough still deserve structured evaluation.
Why Can LPR Damage the Throat Without Burning the Chest?
The larynx and nearby tissues are less equipped than the lower esophagus to tolerate repeated exposure to acidic and enzyme-rich material. In research literature, pepsin is frequently discussed because it can remain biologically relevant even when full acidity is not present. A mechanistic overview in a peer-reviewed review on refluxate injury describes how acid, pepsin, and bile components may contribute to inflammatory and mucosal effects in upper airway tissues.
Experimental and translational evidence, including work summarized on pepsin-mediated injury pathways, suggests that repeated low-volume episodes may still produce meaningful symptoms over time. This helps explain why patients with relatively subtle reflux episodes can still develop ongoing hoarseness or chronic throat irritation even without dramatic heartburn.
Another reason the condition feels "silent" is symptom timing. Patients may notice voice fatigue in the morning, nighttime cough, or a persistent need to clear the throat rather than immediate post-meal burning. Sleep behavior, meal timing, and body position can all influence this pattern. If you are already working on circadian stability and sleep quality, structured habits from this sleep improvement guide can complement reflux-specific measures.
Symptoms, Patterns, and Red Flags You Should Not Ignore
No single symptom confirms LPR. Instead, clinicians look for patterns that persist despite hydration, voice rest, and basic respiratory care. Common complaints include chronic throat clearing, intermittent hoarseness, chronic dry cough, globus sensation, mild swallowing discomfort, excess throat mucus, and voice changes after meals or when waking. Symptom burden often fluctuates with stress, meal composition, and sleep position.
The Reflux Symptom Index, published in a validated symptom scoring study, is often used as a structured way to track symptom severity over time. It is not a stand-alone diagnosis tool, but it helps improve follow-up quality by giving both patient and clinician a shared measurement language.
Some patients also report overlap with digestive bloating, irregular bowel habits, and food sensitivity patterns. In those situations, addressing gut ecosystem factors may be useful in parallel. Practical gut-support reading includes probiotic strains and evidence and microbiome personalization basics. These do not replace reflux care, but they can strengthen broader digestive resilience.
| Symptom Pattern | How Often It Appears in LPR Workups | Clinical Implication |
|---|---|---|
| Morning hoarseness | Common | Suggests overnight reflux exposure and sleep-position influence |
| Frequent throat clearing | Common | Can reflect laryngeal irritation but also allergy or postnasal drip |
| Chronic cough with normal chest imaging | Frequent in referral settings | Consider reflux among causes after pulmonary causes are addressed |
| Globus sensation | Very common | Nonspecific, but helpful when combined with other reflux-linked symptoms |
Urgent red flags: progressive swallowing difficulty, painful swallowing, coughing blood, unexplained persistent weight loss, neck mass, persistent unilateral ear pain, or lasting voice change beyond a few weeks. These signs require prompt in-person ENT or GI evaluation because they can reflect conditions beyond reflux.
How Clinicians Diagnose LPR and Where Tests Help Most
Diagnosis is usually layered, not binary. A typical sequence includes clinical history, symptom scoring, laryngeal examination, and selective reflux testing. Laryngoscopic scoring frameworks such as the Reflux Finding Score from this foundational publication are useful for structured documentation, but findings can overlap with infection, allergy, voice overuse, and irritant exposure.
Objective testing can improve confidence in selected patients, especially those with persistent symptoms, atypical presentations, or poor response to initial therapy. Depending on local expertise, this may include ambulatory pH monitoring or impedance-pH testing. The main point is not to test everyone immediately, but to avoid long-term empiric treatment without reassessment when progress is limited.

| Diagnostic Tool | What It Adds | Main Limitation |
|---|---|---|
| Symptom questionnaires | Tracks severity trends and treatment response over time | Symptoms are not specific to reflux |
| Laryngoscopy | Direct visualization of laryngeal findings | Inter-observer variability and overlap with other causes |
| Ambulatory pH or impedance-pH monitoring | Provides objective reflux burden data | Availability, cost, interpretation complexity |
| Empiric treatment trial with follow-up | Pragmatic when symptoms are typical and red flags absent | Can delay alternate diagnoses if not reassessed systematically |
When cough is prominent, reflux may be one of several contributors. Upper-airway cough syndrome, asthma spectrum disease, medication effects, and chronic sinus issues should still be evaluated. A clean chest workup does not prove reflux, but persistent throat-plus-cough symptoms with meal and posture triggers increase suspicion.
Myth vs Fact: LPR Claims the Evidence Supports and Rejects
Myth: "If I do not feel heartburn, it cannot be reflux." Fact: extra-esophageal reflux can occur with little chest burning. This is one reason LPR evaluation often starts in ENT clinics.
Myth: "One normal scope means reflux is impossible." Fact: reflux-related symptoms fluctuate, and no single test perfectly captures all episodes. Diagnosis is stronger when symptom patterns, structured exam findings, and objective testing align.
Myth: "Medication alone solves every case." Fact: outcomes improve when medication is paired with meal timing, trigger reduction, sleep-position strategy, and periodic reassessment. In persistent cases, objective testing can prevent unnecessary prolonged drug exposure.
Myth: "Surgery is the automatic next step if pills are not ideal." Fact: procedural options are selective and should follow careful phenotyping. Data such as fundoplication outcome analyses show that not all LPR-dominant patients benefit equally, especially when objective reflux evidence is weak.
Myth: "All cough in reflux patients is from acid." Fact: cough can be multifactorial. Reflux may coexist with airway hypersensitivity, allergic inflammation, or sinus disease. This is why integrated care often outperforms single-specialty treatment.
Treatment Ladder: From Food and Sleep to Medication
A practical treatment plan is staged. Stage 1 focuses on behavior and exposure reduction. Stage 2 adds targeted medications when needed. Stage 3 involves specialist-level re-evaluation and, in selected cases, procedural care. The largest long-term gains usually come from consistent day-to-day behaviors.
Guideline-aligned lifestyle measures include avoiding very late meals, reducing large high-fat evening portions, limiting alcohol and nicotine exposure, moderating highly acidic triggers, and elevating the head of bed for nighttime symptoms. Classic data on head-of-bed elevation from randomized positional research supports posture as a low-risk intervention that can reduce nocturnal exposure in suitable patients.
| Step | Core Actions | How to Evaluate Progress |
|---|---|---|
| Step 1: Exposure control | Meal timing, trigger reduction, sleep-position strategy, hydration, voice hygiene | 2-4 week symptom log with consistent scoring |
| Step 2: Medication trial | Clinician-directed acid suppression and symptom-tailored adjuncts | 4-12 week reassessment with explicit goals |
| Step 3: Re-phenotype | Objective reflux testing and alternative diagnosis review | Decide whether to de-escalate, continue, or change strategy |
| Step 4: Procedure-level consideration | Selected surgical/endoscopic options in properly characterized cases | Shared decision based on risks, expected benefit, and evidence fit |
Medication strategy should always be individualized. Overly long empiric therapy without review can hide diagnostic uncertainty. If a patient improves partially but not completely, that is often the right moment to revisit diagnosis rather than automatically escalating dose indefinitely. In parallel, digestive support practices such as food-quality upgrades and strain-specific probiotic selection may help some people improve meal tolerance. See probiotics benefits and side-effect profile and probiotic foods versus supplements for practical context.
A 7-Day LPR-Friendly Meal and Habit Framework
The goal is not a perfect elimination diet forever. The goal is symptom stabilization, then careful reintroduction. Many patients do best with a 2- to 4-week structured window where they simplify meals, control portion size at night, reduce known triggers, and track symptoms objectively. After stabilization, foods can be reintroduced one at a time.
Use this framework as a behavioral template. If you have diabetes, kidney disease, pregnancy, or complex medication regimens, adapt with your clinician or dietitian.
| Common Trigger Pattern | Lower-Irritation Swap | Why It Helps |
|---|---|---|
| Late heavy fried dinner | Earlier meal with lean protein and cooked vegetables | Lower fat load and longer upright window before sleep |
| Tomato-chili-citrus concentrated sauces at night | Herb-forward, lower-acid sauces or broth-based options | Reduces acidic exposure during vulnerable nighttime period |
| Alcohol near bedtime | Alcohol-free evenings during symptom-reset phase | May reduce sphincter relaxation and mucosal irritation |
| Large dessert plus lying down quickly | Smaller earlier snack and 2-3 hour upright interval | Reduces post-meal reflux opportunity |
7-day implementation sequence: Days 1-2 establish meal timing and remove late-night triggers. Days 3-4 standardize breakfast and lunch around low-irritation foods and hydration. Days 5-6 optimize sleep posture and evening routine. Day 7 review symptom log and identify highest-value habits for the next week. This cadence keeps the plan realistic while generating enough data for meaningful follow-up.
If symptom burden improves, continue for another week and begin careful food reintroduction. If no meaningful improvement occurs despite adherence, that is useful information and a reason to escalate diagnostic precision rather than self-restricting indefinitely.
Special Populations: Pregnancy, Children, and Older Adults
Pregnancy: reflux symptoms are common during pregnancy due to hormonal and mechanical factors. Management should prioritize conservative strategies first, then medication only with obstetric guidance. Lifestyle and positioning are especially important in this period.
Children: symptom interpretation is harder because hoarseness, cough, or feeding aversion can have multiple causes. Pediatric evaluation should avoid over-diagnosis and over-treatment while still addressing significant feeding or respiratory impacts.
Older adults: multimorbidity and polypharmacy raise the stakes. Persistent throat symptoms may be attributed to age or chronic sinus issues when reflux is present, or reflux may be blamed when another diagnosis is responsible. Medication risk-benefit review should be explicit in this group.
Across all populations, durable outcomes come from periodic reassessment, not one-time labeling. If symptoms change pattern, worsen rapidly, or include red flags, re-evaluation should happen quickly.

How to Track Progress Over 30 Days Without Guessing
Many treatment plans fail because patients and clinicians are both reacting to memory instead of trend data. A structured 30-day log can change that. Choose three to five daily markers, keep them consistent, and score them at the same time each day. Useful markers include throat-clearing frequency, morning voice quality, nighttime awakenings from cough, globus severity, and post-meal discomfort. Add one behavior score for adherence to meal timing and bedtime spacing.
By week two, patterns often emerge. For example, some people discover that symptom spikes follow late meals much more than spicy foods, while others notice alcohol or carbonated drinks as the bigger trigger. This lets you make targeted changes instead of broad restrictions. It also helps during specialist visits because you can show objective trend lines instead of recalling scattered bad days.
A practical review schedule is simple: at day 7, confirm adherence basics; at day 14, adjust the top two triggers; at day 21, evaluate whether symptom reduction is clinically meaningful; at day 30, decide whether to continue current strategy, step up testing, or de-escalate medications. If you are not improving after strong adherence, that is valuable diagnostic information and a reason to pursue objective testing rather than indefinitely extending empiric treatment.
This process also protects against overtreatment. If symptoms improve clearly with behavior and time-limited medication, you can discuss careful step-down rather than staying at high intensity by default. If symptoms remain unstable despite adherence, you can escalate with better confidence that the next step is justified.
Frequently Asked Questions
Can silent reflux happen even if I never feel heartburn?
Yes. Many LPR patients report throat-focused symptoms with little or no chest burning. A symptom pattern that includes chronic throat clearing, morning hoarseness, cough, and meal or posture triggers can still be reflux-related.
How long does it usually take to feel better after starting treatment?
Some people notice initial improvement in a few weeks, but meaningful stabilization often takes longer because mucosal irritation and behavior patterns need time to recover. Tracking symptoms with a structured score is more reliable than relying on day-to-day impressions.
Do I need a strict diet forever?
Usually no. Most evidence-based approaches use a structured short reset period, then gradual food reintroduction guided by symptom response. The goal is identifying your highest-impact triggers, not maintaining unnecessary long-term restriction.
When should I ask for reflux monitoring instead of another medication trial?
If symptoms persist despite a well-executed lifestyle and medication plan, or if your symptom profile is atypical, objective testing can clarify whether reflux burden is truly driving symptoms. This can prevent prolonged treatment mismatch.
Can surgery cure silent reflux?
Procedure-level options can help selected patients, but they are not universal solutions. Benefit is more likely when objective reflux evidence is strong and symptom phenotype matches what surgery can improve.
Key Takeaways for Long-Term Control
Silent acid reflux is manageable, but it usually requires better pattern recognition than classic heartburn. The best outcomes come from a combined approach: symptom tracking, trigger control, sleep-position strategy, evidence-based medication use when needed, and structured reassessment if progress stalls. If your symptoms are persistent or include red flags, seek timely ENT or GI care for a targeted diagnostic plan.
Related Articles
- Probiotic Strains and Species Benefits Research - A practical review of how different strains affect digestive and immune outcomes.
- Health Benefits of Probiotic Foods and Supplements - Compares food-first and supplement-first strategies for gut support.
- Best Ways to Improve Your Sleep - Useful sleep-habit upgrades that also support nighttime reflux control.
- Gut Health Personalization and Microbiome Testing - Explains when personalized gut approaches can add value to symptom management.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.