
Leaky Gut Syndrome — Symptoms, Causes, and Evidence-Based Healing
Learn what intestinal permeability means, which symptoms to watch for, and evidence-based strategies to support gut barrier repair and digestive health.
12 Min Read
What Your Gut Barrier Actually Does
Your intestinal lining has a contradictory job. It needs to let nutrients through (water, vitamins, amino acids, fatty acids) while keeping bacteria, toxins, and undigested food particles out of your bloodstream. That balancing act, called selective permeability, is what keeps you healthy.
The barrier works through four defensive layers: a microbial layer where trillions of bacteria crowd out pathogens, a biochemical layer of mucus and antimicrobial peptides, a physical layer of epithelial cells locked together by protein complexes, and an immune layer of specialized cells watching for threats.
Quick fact: Your gut houses over 100 trillion bacteria with roughly 1.5 kg of combined biomass. Over 200 microbial strains inhabit a single person's intestines, with more than 90% belonging to the Firmicutes and Bacteroidetes phyla.
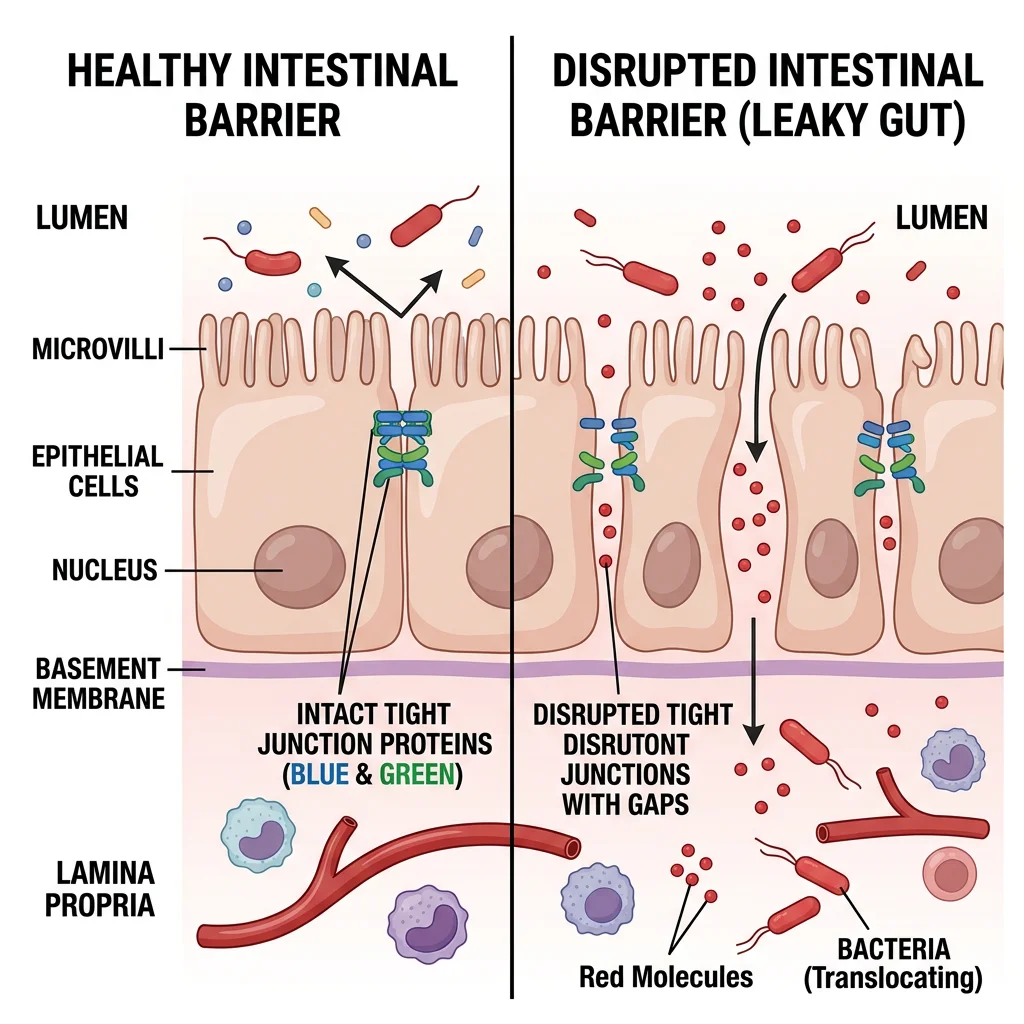
The physical barrier is just a single layer of epithelial cells, but it replaces itself every 3 to 5 days, making it one of the fastest-renewing tissues in the body. These cells connect through protein structures called tight junctions, which control what passes between them. The main tight junction proteins include occludin, claudins, junctional adhesion molecules (JAMs), and zonula occludens (ZO) proteins.
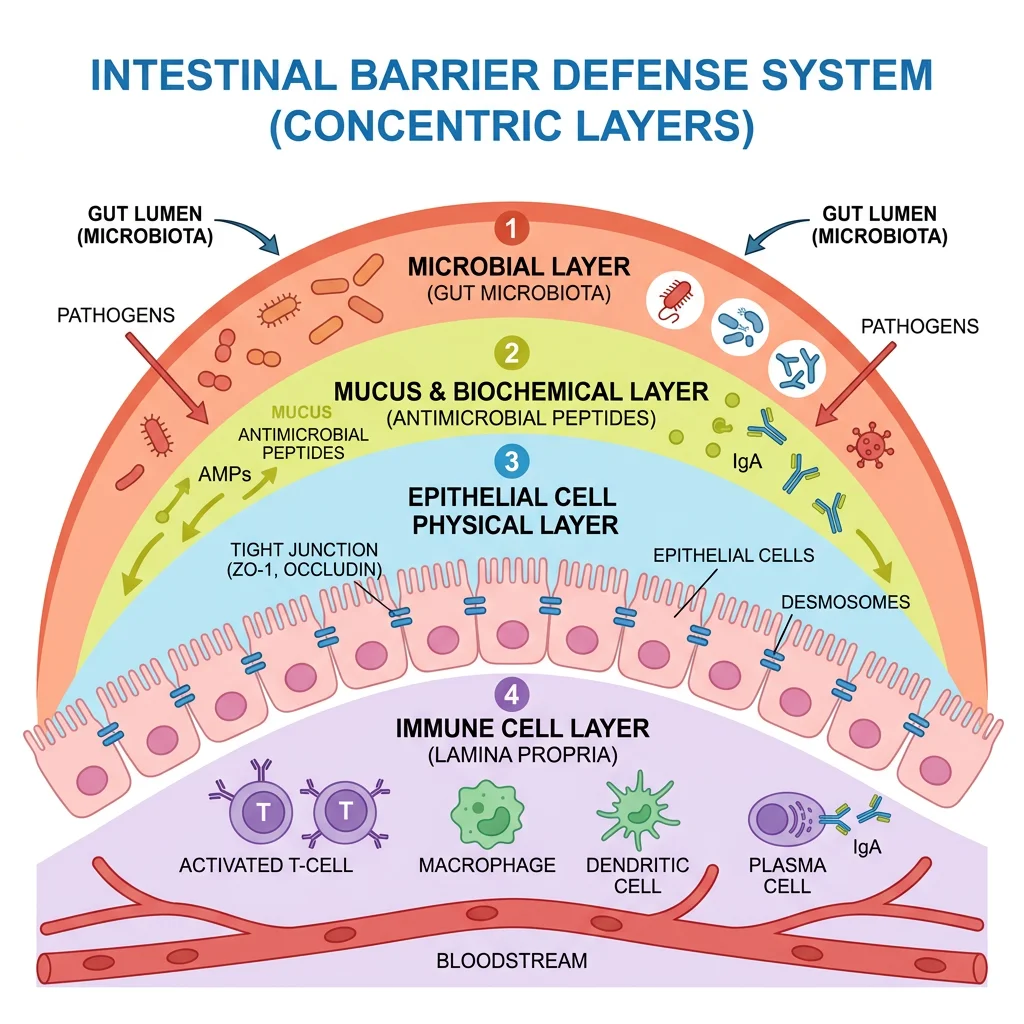
The colonic mucus layer alone can exceed 800 microns in thickness. That's a serious buffer zone keeping bacteria physically separated from the epithelial surface. When everything works properly, roughly 90% of antigens cross the epithelium through regulated transcellular pathways, with only about 10% passing between cells as intact proteins.
When the Barrier Breaks Down: What "Leaky Gut" Really Means
When tight junctions loosen or the mucus layer thins, molecules that normally stay in the intestinal tract start crossing into the bloodstream. This is increased intestinal permeability, or what popular health media calls "leaky gut syndrome."
One thing to get straight: leaky gut is not a recognized medical diagnosis. Gastroenterologists and researchers agree that increased intestinal permeability is a real, measurable phenomenon. They can detect it using lactulose-to-mannitol ratio tests, confocal laser endomicroscopy, and other methods. But "leaky gut syndrome" as a standalone disease with its own diagnostic criteria and treatment protocols? That doesn't exist in medical literature.
This matters for treatment. Increased permeability appears to be a feature of many diseases, including inflammatory bowel disease, IBS, celiac disease, type 1 diabetes, obesity, and heart disease, rather than a disease that causes them. The relationship between barrier dysfunction and these conditions runs both ways, and researchers haven't fully untangled it.
Researchers describe autoimmune disease development through a "three-legged stool" model: genetic susceptibility, an environmental trigger, and loss of barrier function. All three appear necessary. Barrier impairment on its own does not seem to be enough. Less than 10% of people with genetic susceptibility to autoimmune conditions actually develop clinical disease.
Symptoms That May Signal Increased Intestinal Permeability
No symptom is unique to intestinal permeability problems. That's the frustrating part. The symptoms people attribute to leaky gut overlap heavily with IBS, functional dyspepsia, food intolerances, and dozens of other gastrointestinal conditions.
That said, research has identified symptoms that frequently show up alongside measurably increased permeability:
| Symptom Category | Specific Symptoms | Notes |
|---|---|---|
| Digestive | Bloating, gas, diarrhea, constipation | 18% of the global population reports weekly bloating; over 70% of IBS patients report it |
| Systemic | Fatigue, brain fog, joint pain | Often attributed to systemic inflammation from translocated endotoxins |
| Skin | Eczema, rashes, acne | Gut-skin axis research links barrier dysfunction to inflammatory skin conditions |
| Immune | Frequent infections, food sensitivities | 61% of IBS patients showed epithelial gaps within 5 minutes of food antigen exposure |
| Metabolic | Blood sugar fluctuations, weight changes | Hyperglycemia itself drives barrier permeability via GLUT2 reprogramming |
The Cleveland Clinic's position is direct: no symptoms are directly and uniquely attributable to intestinal permeability. If you have persistent digestive symptoms, work with a gastroenterologist to rule out diagnosable conditions before assuming leaky gut is the explanation.
What Damages the Gut Barrier?
Barrier breakdown rarely comes from one thing. More often, it's a combination of diet, medications, stress, and environmental exposures wearing down your gut's ability to keep up with repairs.
Dietary Factors
Diets heavy in refined sugar, processed carbohydrates, and omega-6 fatty acids while low in fiber create conditions that weaken the barrier. High-fat diets alter tight junction protein expression and promote endotoxemia, the leakage of bacterial toxins into the bloodstream. Dietary emulsifiers in processed foods, including carboxymethylcellulose (CMC) and polysorbate 80, compromise the mucus layer that protects the epithelium.
Medications
NSAIDs like ibuprofen and naproxen are well-documented barrier disruptors. One study found that zinc carnosine at 37.5 mg twice daily could prevent the permeability increase that NSAIDs typically cause. Antibiotics, proton pump inhibitors (PPIs), and certain psychotropic medications also change microbiota composition and barrier function.
Alcohol
Alcohol and its metabolites are directly toxic to intestinal epithelial cells. This isn't limited to heavy drinking. Even moderate consumption affects barrier integrity.
Environmental Exposures
Several environmental threats have emerged in recent research. Microplastics damage the intestinal barrier and reduce mucus production. Nanoparticles destabilize mitochondrial function and disrupt cell connections. Even household detergents and cleaning chemicals can damage tight junctions on contact.
Stress and Circadian Disruption
Psychological stress measurably increases intestinal permeability. This has been demonstrated in both animal models and human studies. Permeability also follows a circadian cycle, so disrupted sleep patterns can make things worse. If you work nights or travel across time zones regularly, your gut barrier may be more vulnerable than someone who keeps a consistent sleep schedule.
| Barrier Disruptor | Mechanism | Reversibility |
|---|---|---|
| Processed food emulsifiers | Thin the protective mucus layer | Reversible with dietary changes |
| NSAIDs | Direct epithelial damage | Reversible upon cessation; zinc carnosine may protect |
| Alcohol | Toxic to epithelial cells | Reversible with abstinence |
| Chronic stress | Cortisol-mediated tight junction loosening | Reversible with stress management |
| Microplastics | Physical barrier damage, mucus reduction | Limited data on reversibility |
| Antibiotics | Microbiome disruption, indirect barrier weakening | Partially reversible; recovery takes weeks to months |
The Zonulin Connection: How Gluten and Bacteria Trigger Permeability
In 2000, researcher Alessio Fasano identified a protein called zonulin, the only known physiological modulator of intestinal tight junctions. Zonulin is a 47 kDa protein (specifically, pre-haptoglobin 2) that reversibly regulates tight junction permeability when released by intestinal cells.
Two things trigger zonulin release: exposure to certain gut bacteria and exposure to gliadin, the protein fraction of gluten. When gliadin reaches the intestinal surface, it binds to a chemokine receptor called CXCR3 on epithelial cells. That kicks off a signaling cascade where gliadin activates PAR2, which transactivates the epidermal growth factor receptor (EGFR), and tight junctions start to come apart.
The zonulin data across diseases is pretty telling. In active celiac disease, 81% of patients show elevated zonulin levels, and even 50% of their first-degree relatives who don't have celiac show elevations. In type 1 diabetes, 42% of patients have elevated zonulin, with 29% of relatives affected. Elevated zonulin has also been documented in rheumatoid arthritis, multiple sclerosis, ankylosing spondylitis, and obesity.
Where it gets complicated: research using transgenic mouse models suggests that dysregulated zonulin may itself cause dysbiosis, an imbalance in gut bacteria. So zonulin doesn't just respond to bacterial triggers. It may also reshape the bacterial environment. The relationship goes both ways.
A drug called larazotide acetate (AT1001), designed to block zonulin's action, reduced type 1 diabetes incidence by 70% in a rat model. Human trials for celiac disease showed promising results in reducing symptoms and permeability, though the drug hasn't reached widespread clinical use.
A caveat on testing: Commercial zonulin blood tests marketed directly to consumers have significant methodological problems. A 2024 review found that many available assays do not actually measure zonulin specifically, making at-home or direct-to-consumer zonulin tests unreliable for clinical decision-making.
Myth vs. Fact: Separating Science from Supplement Marketing
There's a wide gap between what research shows and what supplement companies claim. The evidence tells a different story than the labels do.
| Claim | What the Evidence Says | Verdict |
|---|---|---|
| "Leaky gut causes autoimmune disease" | Barrier dysfunction is ONE of three necessary factors (with genetics and environmental triggers). Less than 10% of genetically susceptible people develop autoimmune disease. | Oversimplified |
| "You can diagnose leaky gut with a blood test" | Commercial zonulin assays are methodologically flawed. Lactulose-mannitol ratio testing requires clinical supervision. | Misleading |
| "Eliminating gluten heals leaky gut for everyone" | Gliadin triggers zonulin release, but this is most relevant for celiac patients and a subset of IBS patients. Universal gluten avoidance is not supported. | Partially true, overgeneralized |
| "Bone broth seals a leaky gut" | No controlled human trials support bone broth specifically for intestinal permeability. Glutamine (found in broth) has some evidence, but at higher doses than broth provides. | Unproven |
| "Probiotics fix leaky gut" | Specific strains (Bifidobacterium species and E. coli Nissle 1917) have shown permeability improvements in targeted studies. No probiotic has been studied for "leaky gut" as a standalone condition. | Strain-specific, not universal |
The supplement industry has turned intestinal permeability into a marketing angle, but researchers are more cautious. The Cleveland Clinic says the only proven approach is treating the underlying condition causing the permeability increase, not taking supplements marketed for "leaky gut."
Evidence-Based Strategies to Support Gut Barrier Repair
Several interventions do have real research behind them. None of them will fix everything overnight, but each has shown measurable effects on intestinal permeability in controlled studies.
Glutamine Supplementation
Glutamine is the primary fuel source for intestinal epithelial cells. In a randomized controlled trial of patients with post-infectious IBS-D, glutamine at 5 grams three times daily improved the lactulose-to-mannitol ratio, which is a direct measure of intestinal permeability. As far as supplements for barrier function go, this is the strongest human trial data available.
Zinc Carnosine
Zinc carnosine at 37.5 mg twice daily prevented NSAID-induced permeability increases in a controlled study. If you take anti-inflammatory medications regularly and worry about gut barrier integrity, this is worth bringing up with your doctor.
Vitamin D
Vitamin D3 at 2,000 IU per day maintained intestinal permeability in Crohn's disease patients who were in remission. Vitamin D receptors are expressed throughout the intestinal epithelium, and deficiency has been linked to barrier dysfunction in multiple studies. If you're looking to strengthen your immune system naturally, getting your vitamin D levels checked is a reasonable place to start.
Targeted Probiotics
Not all probiotics are equal for barrier function. Bifidobacterium strains specifically reduced permeability in a study of obese adults. E. coli Nissle 1917 was shown to stimulate ZO-2 protein expression, one of the key tight junction components. Polyphenols and omega-3 fatty acids have also shown tight junction-strengthening effects in research settings.

Exclusion Diets (With Medical Supervision)
Research from Mayo Clinic found that IBS patients on a gluten-containing diet had greater small bowel permeability with decreased expression of ZO-1, claudin-1, and occludin. Using confocal laser endomicroscopy, researchers observed epithelial gaps forming within 5 minutes of food antigen exposure in 61% of IBS patients tested. Exclusion diets produced over 50% symptom improvement at 4 weeks and 74% improvement at 12 months.
A low-FODMAP diet, which cuts fermentable carbohydrates that can trigger symptoms, has shown particular benefit for IBS patients with barrier dysfunction. Good nutrition matters to both barrier repair and overall immune resilience.
Foods That Strengthen vs. Weaken the Intestinal Barrier
What you eat has a direct, measurable impact on tight junction integrity. The research on specific foods is clearer than you might expect.
Barrier-Strengthening Foods
Fermentable fibers from vegetables, legumes, and whole grains improve barrier function through short-chain fatty acid (SCFA) production. When gut bacteria ferment these fibers, they produce butyrate, propionate, and acetate. These SCFAs nourish colonocytes and reinforce tight junctions. Probiotic-rich fermented foods also add beneficial bacteria that compete with pathogens along the intestinal lining.
Polyphenol-rich foods like berries, green tea, dark chocolate, and olive oil strengthen tight junction integrity through multiple mechanisms. Omega-3 fatty acids from fatty fish, flaxseed, and walnuts also support barrier function.
Barrier-Weakening Foods
Ultra-processed foods are the biggest dietary threat to gut barrier health, mostly because of their additives. Emulsifiers like carboxymethylcellulose and polysorbate 80, found in ice cream, salad dressings, and many packaged foods, directly compromise the mucus barrier protecting the epithelium. High-sugar and high-refined-carbohydrate diets feed bacterial populations that produce barrier-damaging metabolites.

| Barrier-Strengthening | Mechanism | Barrier-Weakening | Mechanism |
|---|---|---|---|
| Fermentable fibers (legumes, oats) | SCFA production nourishes colonocytes | Refined sugars, processed carbs | Feed harmful bacteria, increase endotoxins |
| Polyphenol-rich foods (berries, green tea) | Strengthen tight junction proteins | Food emulsifiers (CMC, polysorbate 80) | Thin the protective mucus layer |
| Omega-3 sources (fatty fish, flaxseed) | Anti-inflammatory, support tight junctions | High omega-6 oils (soybean, corn oil) | Pro-inflammatory, disrupt barrier signaling |
| Fermented foods (yogurt, kimchi, sauerkraut) | Provide beneficial probiotic bacteria | Alcohol | Directly toxic to epithelial cells |
| Glutamine-rich foods (chicken, fish, cabbage) | Fuel for epithelial cell repair | High-fat meals | Alter tight junction proteins, promote endotoxemia |
Frequently Asked Questions
Is leaky gut a real medical condition?
Increased intestinal permeability is real and measurable. Researchers can detect it using tests like the lactulose-to-mannitol ratio. But "leaky gut syndrome" is not a recognized medical diagnosis with established diagnostic criteria. It's a descriptive term for a process that occurs across many different diseases, not a standalone condition.
How long does it take to heal a leaky gut?
The intestinal epithelium renews itself every 3 to 5 days, so physical repair can begin quickly once the damaging factor is removed. In studies using exclusion diets, over 50% of patients reported symptom improvement within 4 weeks, and 74% showed improvement at 12 months. The timeline depends entirely on the underlying cause.
Should I take a zonulin test to check for leaky gut?
Commercial zonulin tests marketed to consumers have significant reliability problems. A 2024 review found that many commercially available assays don't specifically measure zonulin, making the results hard to interpret clinically. Work with a gastroenterologist who can order validated testing rather than relying on direct-to-consumer kits.
Can probiotics help with intestinal permeability?
Certain strains have shown benefit in controlled studies. Bifidobacterium species reduced permeability in obese adults, and E. coli Nissle 1917 stimulated tight junction protein expression. But benefits are strain-specific. A generic probiotic supplement may not contain the strains that have shown barrier effects in clinical trials.
Does gluten cause leaky gut in people without celiac disease?
Gliadin, the protein fraction in gluten, triggers zonulin release in intestinal cells regardless of celiac disease status. But the clinical significance varies from person to person. Research from Mayo Clinic found that IBS patients on a gluten-containing diet had measurably greater intestinal permeability. For the general population without IBS or celiac disease, the evidence for universal gluten avoidance is not strong.
Related Articles
- Health Benefits of Probiotics: An Evidence-Based Ultimate Guide — A deep look at the science behind probiotics, including strain-specific benefits for digestive and immune health.
- Do Probiotics for Celiac Disease Contain Gluten? — If you have celiac disease and are considering probiotics to support gut healing, this guide covers what to watch for.
- Natural Ways to Strengthen Your Immune System — Gut health is the foundation of immune function. Explore evidence-based strategies to support both.
- Nutrition for a Stronger Immune System — How the right dietary choices support both barrier integrity and immune resilience.
- Immune-Boosting Probiotic Foods — Fermented foods that deliver barrier-supporting bacteria directly to your gut.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.