
Iron Deficiency in Women: Symptoms, Testing, and Recovery
Learn the signs of iron deficiency in women, which blood tests to request, and evidence-based strategies for restoring your iron levels safely.
12 Min Read
The short version: Iron deficiency is the most common nutritional deficiency worldwide, and women of reproductive age get hit hardest. Your body needs iron to carry oxygen, produce energy, and keep your brain working. If you are constantly tired, losing hair, craving ice, or getting dizzy, your iron levels may be low enough to cause real problems. A blood test measuring ferritin, hemoglobin, and transferrin saturation can confirm it. Recovery is slow — most women need 6 to 7 months of steady supplementation to fully rebuild their iron stores.
Your Body Runs on Iron — and Women Spend It Faster
Iron sits at the center of hemoglobin, the protein in red blood cells that carries oxygen from your lungs to every tissue in your body. Without enough of it, your cells starve for oxygen. Muscles weaken. Thinking gets foggy. Your heart starts working harder to compensate.
Women lose iron in ways men don't. Menstruation alone drains roughly 1 mg of iron per day of bleeding, according to the National Institutes of Health Office of Dietary Supplements. Heavy periods push that number higher. Pregnancy demands even more: the recommended daily intake jumps from 18 mg to 27 mg, a 50% increase.
The math is straightforward: premenopausal women need more than double the iron men do. The RDA for women aged 19-50 is 18 mg per day, versus 8 mg for men. After menopause, when menstruation stops, women's needs drop back to 8 mg. If you are somewhere in between, knowing how your body changes during perimenopause can help you plan ahead.
| Life Stage | Iron RDA (mg/day) | Why It Changes |
|---|---|---|
| Girls 14-18 | 15 | Menstruation begins, growth demands |
| Women 19-50 | 18 | Monthly menstrual losses |
| Pregnant women | 27 | Expanded blood volume, fetal demands |
| Breastfeeding | 9-10 | No menstruation offsets milk production |
| Women 51+ | 8 | Menstruation stops |
| Vegetarian women 19-50 | 32 | Plant iron absorbed at lower rates (1.8x multiplier) |
Most women don't come close to meeting their daily target. NHANES data cited by the NIH shows iron deficiency in 9-11% of adolescent girls and reproductive-age women in the United States. Worldwide, iron deficiency without anemia affects roughly 2.4 billion people, making it the most common nutritional deficiency on the planet.
12 Warning Signs Most Women Dismiss as Normal
Iron deficiency doesn't hit you all at once. It builds slowly, showing up as a handful of vague complaints that are easy to blame on stress, bad sleep, or "just getting older." The American Society of Hematology lists the following symptoms:
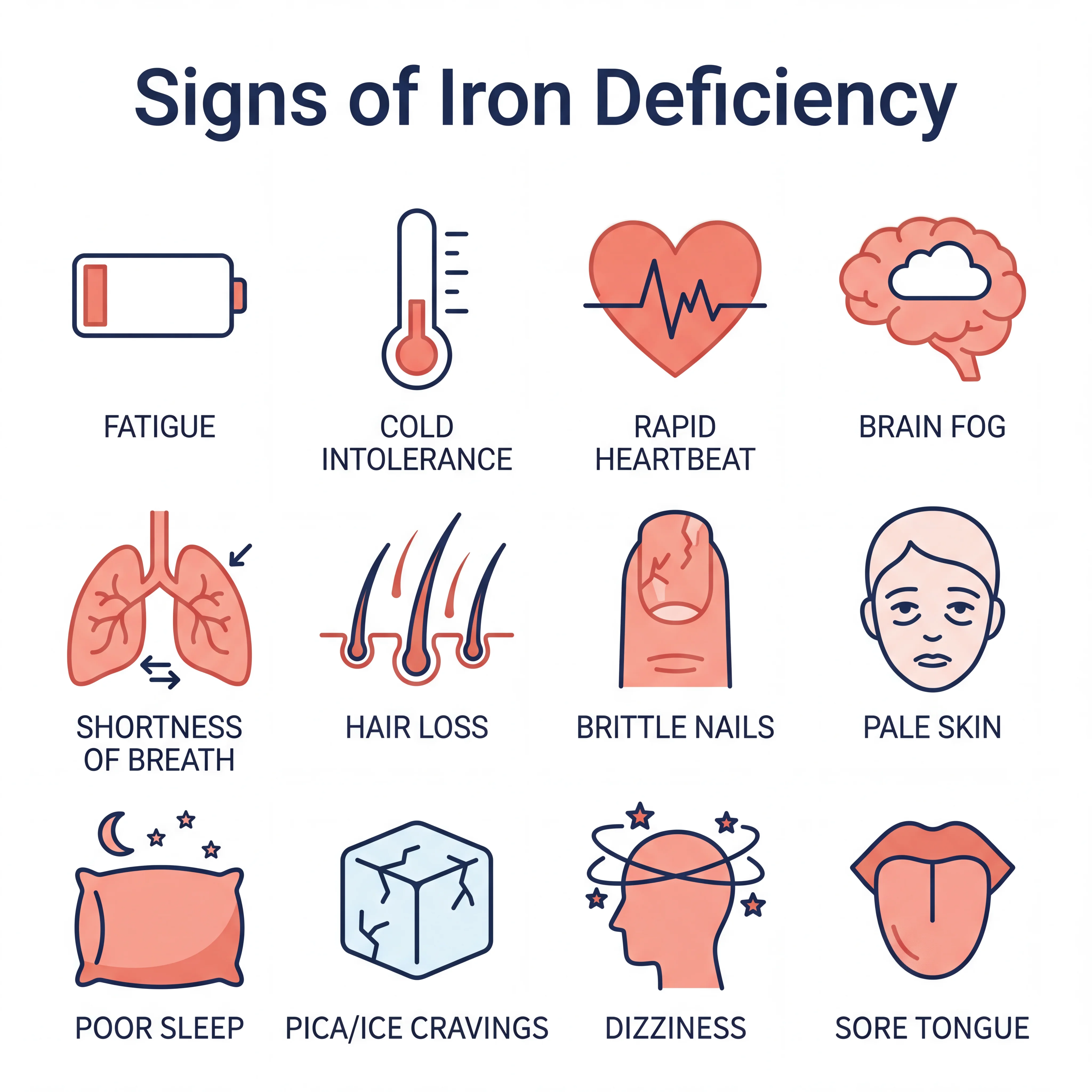
- Unexplained fatigue — the most common complaint, and the easiest to brush off
- Pale or yellowish skin — less hemoglobin means less red color in your blood
- Shortness of breath — your heart and lungs work harder to compensate
- Dizziness or lightheadedness — especially standing up fast
- Rapid or irregular heartbeat — the heart pumps faster when there aren't enough red blood cells
- Cold hands and feet — oxygen isn't reaching your extremities well
- Brittle nails — they may get thin, concave, or ridged
- Hair loss — low iron disrupts the hair growth cycle
- Headaches — worse with physical activity
- Sore or swollen tongue — it may look smooth or unusually pale
- Pica (cravings for ice, clay, or dirt) — strange, but one of the more specific signs
- Restless legs or poor sleep — iron deficiency is a known trigger for restless leg syndrome
If persistent fatigue comes with several of these other signs, get your iron checked before chalking it up to chronic fatigue syndrome or something else entirely.
Iron Depletion Happens in Three Distinct Stages
You don't go from fine to anemic overnight. A clinical review in StatPearls describes iron depletion as a three-stage process, and symptoms can start long before you reach actual anemia.
| Stage | What Happens | Lab Markers | Symptoms |
|---|---|---|---|
| Stage 1: Storage Depletion | Ferritin drops, bone marrow iron decreases | Low ferritin, normal hemoglobin | Often none — may feel mildly tired |
| Stage 2: Functional Iron Deficiency | Circulating iron drops, hemoglobin synthesis slows | Low transferrin saturation, ferritin declining further | Fatigue, brain fog, reduced exercise tolerance |
| Stage 3: Iron Deficiency Anemia | Iron stores exhausted, red blood cells shrink | Low hemoglobin, low MCV, microcytic hypochromic cells | All symptoms above plus pallor, rapid heart rate, shortness of breath |
A lot of women sit in Stage 1 or Stage 2 for months, sometimes years, without knowing it. Iron deficiency without anemia is at least twice as common as iron deficiency with anemia, but it often goes undiagnosed. The reason: standard blood tests may show a "normal" hemoglobin level while ferritin, the actual measure of your iron reserves, is bottomed out.
Women typically store about 300 mg of iron, compared to roughly 1,000 mg in men. That's a thin buffer. One heavy menstrual cycle or a few months of poor intake can tip you into deficiency.
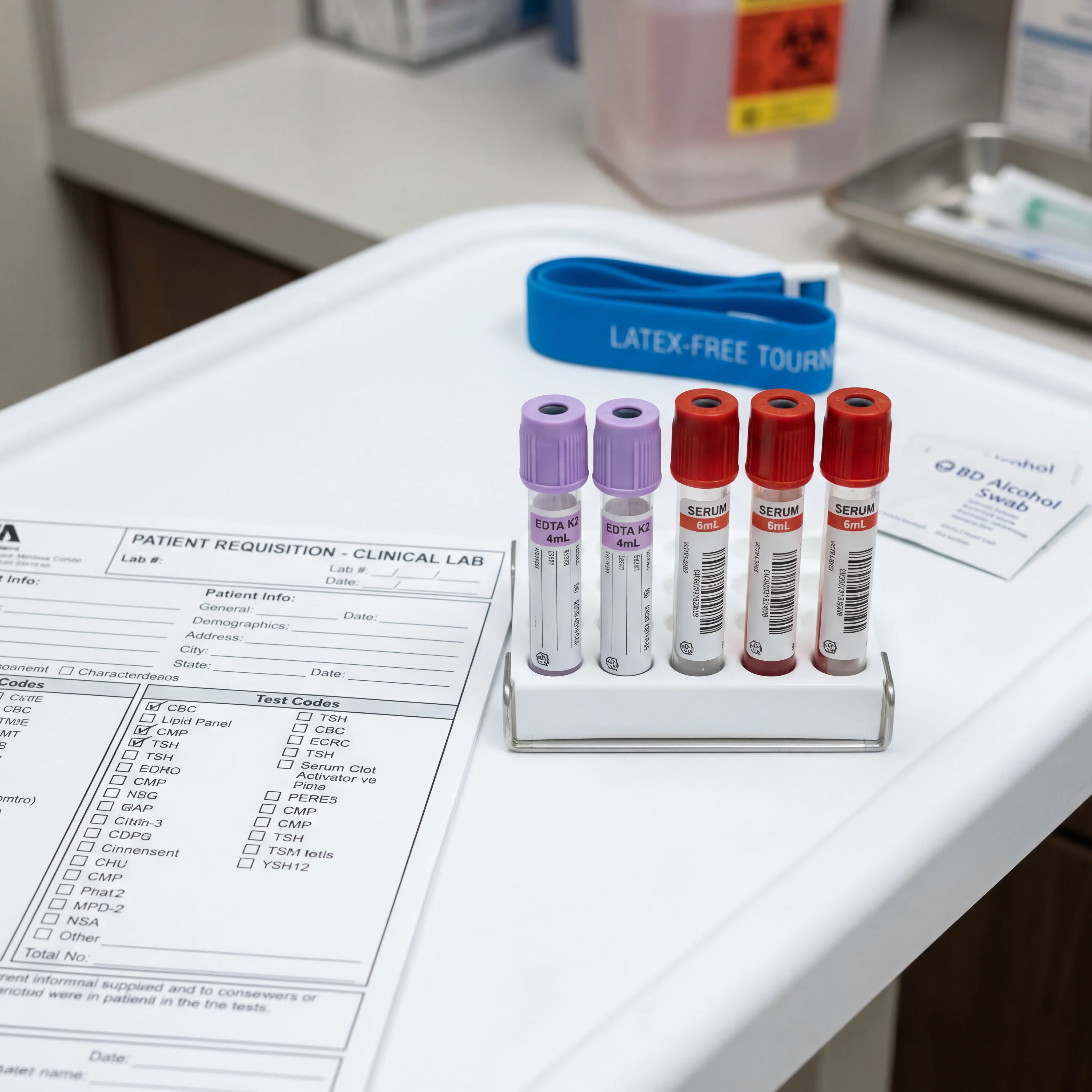
Which Blood Tests to Request and How to Read Them
A CBC by itself won't cut it. Plenty of women with depleted iron stores have a perfectly normal CBC because their hemoglobin hasn't dropped below the threshold yet. If you want to catch iron deficiency early, you need an iron panel that includes ferritin.
| Test | What It Measures | Iron Deficiency Range | Why It Matters |
|---|---|---|---|
| Ferritin | Stored iron | Below 30 mcg/L (deficient); below 45 ng/mL per AGA/ASH for optimal sensitivity | First marker to drop — catches Stage 1 |
| Hemoglobin | Oxygen-carrying capacity | Below 12 g/dL (women); below 11 g/dL (pregnant) | Only drops in Stage 3 (anemia) |
| Transferrin Saturation (TSAT) | Iron available for use | Below 20% | Shows functional iron availability |
| TIBC | Binding capacity (rises when iron is low) | Elevated | Compensatory response to low iron |
| MCV | Red blood cell size | Low (microcytic) | Only abnormal in advanced deficiency |
| Serum Iron | Circulating iron right now | Low | Fluctuates with meals — least reliable alone |
Key takeaway: Ask for ferritin by name. A lot of doctors only order a CBC, which misses Stages 1 and 2 completely. If your ferritin is below 30 mcg/L, you are iron deficient, even if your hemoglobin looks fine. One catch: if you have chronic inflammation (autoimmune disease, infection), the cutoff rises to 100 mcg/L because inflammation artificially inflates ferritin readings.
The technical gold standard is a bone marrow biopsy with iron staining, but that's invasive and rarely needed. In practice, low ferritin plus low transferrin saturation is enough to make the diagnosis.
Myth vs. Fact: What Most People Get Wrong About Iron
There's a lot of bad information about iron floating around. Some of it is harmless. Some of it keeps women from getting help.
| Myth | Fact |
|---|---|
| "Spinach is the best source of iron" | Spinach contains 3 mg per half cup, but its high oxalate content blocks much of the absorption. Oysters (8 mg/3 oz), white beans (8 mg/cup), and beef liver (5 mg/3 oz) deliver more usable iron |
| "If my CBC is normal, my iron is fine" | A normal hemoglobin only rules out Stage 3 anemia. You can be significantly iron deficient with a perfectly normal CBC. You need ferritin tested |
| "All iron supplements are the same" | Ferrous fumarate contains 33% elemental iron, ferrous sulfate 20%, and ferrous gluconate just 12%. The amount of actual iron per pill varies dramatically |
| "Take iron every day for fastest results" | Research shows alternate-day dosing may actually improve absorption because daily doses trigger hepcidin, a hormone that blocks iron uptake for about 24 hours |
| "Cooking in cast iron pans is enough" | Cast iron does leach small amounts of iron into food, but the amount is unpredictable and insufficient to treat a genuine deficiency |
| "Only vegetarians get iron deficient" | While vegetarians need 1.8x more iron due to lower plant-iron bioavailability, any woman with heavy periods, pregnancies, or GI conditions is at risk regardless of diet |
The worst myth on this list might be the unspoken one: that fatigue is "just part of being a woman." It isn't. Persistent exhaustion deserves a blood test, not a shrug. And if you want to eat more iron-rich plants, spinach does have real health benefits, but don't rely on it as your only source.
Which Foods Actually Raise Your Iron Levels
There's a big gap between iron-rich foods that look good on paper and ones your body can actually use. Iron from animal foods (heme iron) is absorbed at rates of 15-35%. Plant iron (non-heme iron) comes in at just 2-20%. Plant sources still count, but you need to think about what you pair them with and how you prepare them.

According to the NIH Office of Dietary Supplements, the highest food sources of iron per serving include:
| Food | Serving | Iron (mg) | Type |
|---|---|---|---|
| Fortified breakfast cereal (100% DV) | 1 serving | 18 | Non-heme |
| Oysters, cooked | 3 oz | 8 | Heme |
| White beans, canned | 1 cup | 8 | Non-heme |
| Beef liver, pan fried | 3 oz | 5 | Heme |
| Lentils, cooked | ½ cup | 3 | Non-heme |
| Spinach, cooked | ½ cup | 3 | Non-heme |
| Tofu, firm | ½ cup | 3 | Non-heme |
| Dark chocolate (45-69% cacao) | 1 oz | 2 | Non-heme |
| Chickpeas, cooked | ½ cup | 2 | Non-heme |
| Beef, braised | 3 oz | 2 | Heme |
Absorption boosters: Vitamin C makes the biggest difference for non-heme iron. Eating citrus, bell peppers, tomatoes, or strawberries with iron-rich plant foods improves uptake noticeably. Meat, poultry, and seafood in the same meal also help.
Absorption blockers: Calcium, tea, coffee, and phytates (in whole grains and legumes) all reduce iron absorption. You don't need to avoid them entirely, but timing matters. If you're supplementing, take your iron away from your morning coffee and any calcium supplements.
Mineral balance plays into this more than most people realize. Understanding how electrolytes interact can help you avoid accidentally blocking iron absorption with poor timing.
Building Your Iron Stores Back: What Recovery Actually Looks Like
For a lot of iron-deficient women, food alone won't get the job done. Supplementation becomes part of the picture, and the approach depends on how depleted you are and whether your stomach can handle oral iron.
Oral iron (first-line treatment):
- Dose: 100-200 mg elemental iron per day, or 28-50 mg daily on alternate days
- Forms: Ferrous sulfate (most studied, least expensive), ferrous fumarate (highest elemental iron per pill), or ferrous gluconate (gentlest on the stomach)
- Vitamin C: Take 250 mg of vitamin C with each iron dose to improve absorption
- Timing: Empty stomach absorbs the most. Keep it 2 hours away from antacids, 4 hours from thyroid medication (levothyroxine), and at least 1 hour from calcium
| Supplement Form | Elemental Iron per Weight | Typical Tablet | Best For |
|---|---|---|---|
| Ferrous sulfate | 20% | 325 mg tablet = 65 mg elemental | First choice, most evidence |
| Ferrous fumarate | 33% | 325 mg tablet = 107 mg elemental | When fewer pills preferred |
| Ferrous gluconate | 12% | 325 mg tablet = 39 mg elemental | Sensitive stomachs |
The side effects are real: nausea, constipation, dark stools, stomach discomfort. But here's something useful. Research suggests that alternate-day dosing may improve absorption while cutting down on side effects. The reason is hepcidin, a liver hormone that kicks in after you take iron and blocks further absorption for about 24 hours. Taking it every other day works with that cycle instead of against it.
Recovery timeline:
- 2-3 weeks: You may start to feel less fatigued
- 1 month: Blood tests should show measurable improvement in hemoglobin
- 3-6 months: Continue supplementation to rebuild stores
- 6-7 months (24-30 weeks): Full iron store replenishment, according to the American Society of Hematology
Don't stop taking iron just because you feel better. Feeling better means your hemoglobin has recovered, but your ferritin stores may still be empty. Aim for a ferritin level of at least 100 mcg/L before you start tapering off.
When IV iron is needed: Oral iron doesn't work for everyone. Your doctor may recommend intravenous iron if you can't tolerate pills, have a malabsorption condition (celiac disease, IBD, post-bariatric surgery), need a fast repletion before surgery, or are in your second or third trimester with significant deficiency. The risk of a severe reaction with modern IV iron formulations is about 1 in 250,000.
Worth noting: your gut health matters here too. Intestinal inflammation can reduce iron absorption even when you're supplementing correctly.
Frequently Asked Questions
Can iron deficiency cause hair loss?
Yes. Iron plays a direct role in the hair growth cycle, and low iron is one of the most common nutritional reasons for hair thinning in women. Ferritin below 30 mcg/L has been linked to increased shedding. Once you restore your iron stores, regrowth usually starts within a few months, but it can take 6-12 months to fully recover.
How long does it take to recover from iron deficiency?
Most women feel less tired within 2-3 weeks of starting supplements. Blood markers start improving within a month. But fully rebuilding your iron stores takes 24-30 weeks (about 6-7 months) of consistent supplementation. Don't stop early. Feeling better doesn't mean your stores are full.
Should I take iron every day or every other day?
Current evidence leans toward alternate-day dosing (like 100 mg every other day) being at least as effective as daily doses, possibly more so. Daily iron triggers hepcidin release, which blocks absorption for roughly 24 hours. Every-other-day dosing lets that window clear, and it tends to cause fewer stomach problems.
Is it possible to take too much iron?
Yes. The tolerable upper limit for adults is 45 mg of elemental iron per day from food and supplements combined. Therapeutic doses for treating deficiency go above that and should be supervised by a doctor. Too much iron (hemochromatosis) can damage your liver, heart, and pancreas. Don't self-treat with high-dose iron without blood work confirming you're actually deficient.
Why does my doctor only test CBC and not ferritin?
Most standard blood panels include a CBC but skip ferritin and iron studies. A CBC only catches Stage 3 (anemia), when hemoglobin has already dropped below normal. To pick up the earlier stages, you need to ask for ferritin and transferrin saturation specifically. If your doctor pushes back, explain your symptoms and request a full iron panel.
Related Articles
- Perimenopause Symptoms and Natural Management Strategies — Hormonal shifts during perimenopause change how you absorb nutrients and manage energy.
- Chronic Fatigue Syndrome: Causes, Symptoms, and Treatment — When the exhaustion isn't coming from low iron.
- Spinach: Health Benefits and Nutritional Facts — What spinach actually delivers beyond the iron reputation.
- Gut Health Personalization and Microbiome Testing — Your gut health affects how well you absorb iron and other minerals.
- Electrolytes: Sodium, Potassium, Magnesium, and Hydration — Mineral interactions that affect iron absorption and energy.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.









