
Menopause Natural Remedies: What Actually Helps Hot Flashes and Sleep
Evidence-based natural remedies for menopause hot flashes and sleep problems. Research-backed options including hypnotherapy, black cohosh, CBT-I, and supplements.
13 Min Read
About 80% of women going through menopause deal with hot flashes. Half of those women also struggle with sleep problems that didn't exist before. And while hormone therapy remains the most effective medical treatment, plenty of women can't take it or would rather not. That leaves a gap between suffering through symptoms and finding non-hormonal options that actually do something.
The natural remedies market doesn't make this easier. Walk into any supplement aisle and you'll count dozens of products promising menopause relief, most backed by little more than a picture of a smiling woman on the label. So what does the clinical research actually support? Below, we sort through the remedies that have real trial data from the ones running on placebo effect and good packaging.
Why Hot Flashes and Sleep Problems Happen During Menopause
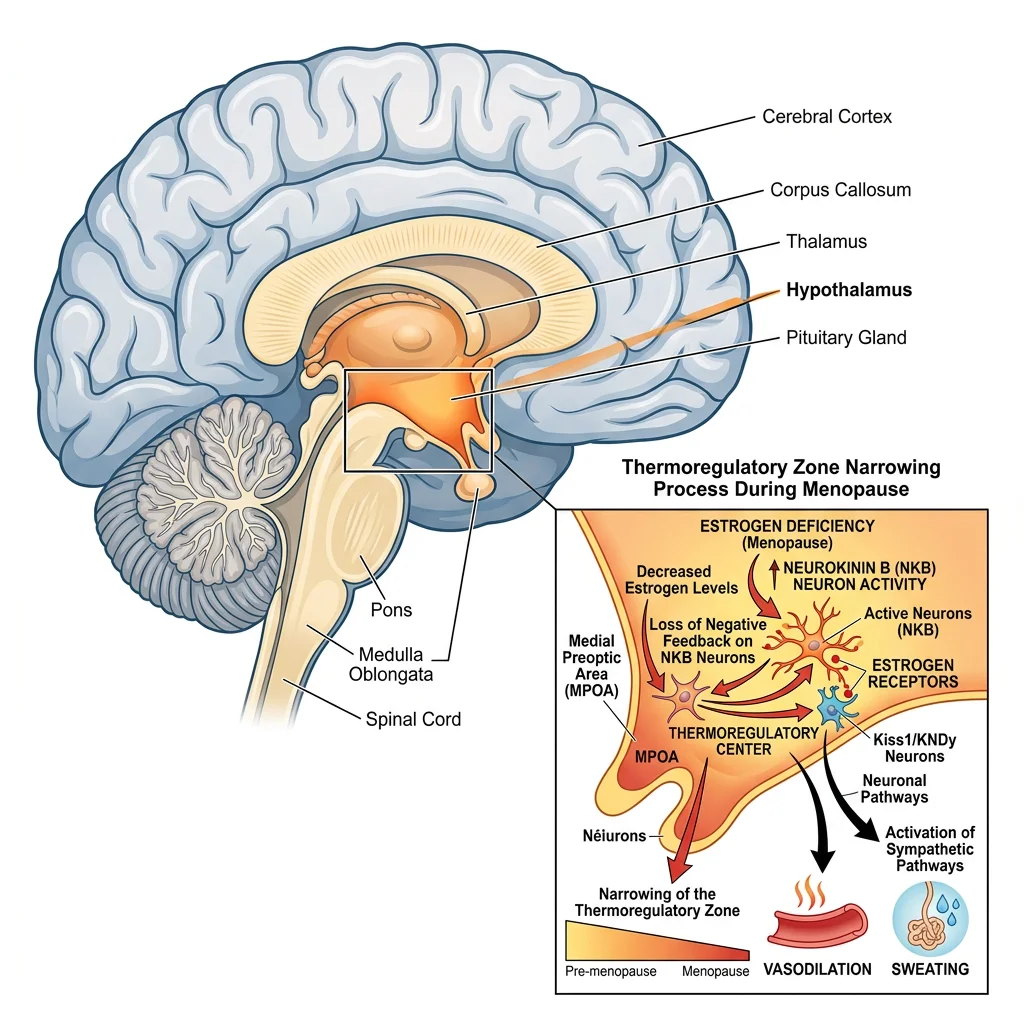
Hot flashes aren't just "feeling warm." They're a measurable physiological event triggered by changes in your brain's thermoregulatory center. As estrogen levels drop during menopause, the hypothalamus becomes more sensitive to small changes in body temperature. The narrowing of the thermoneutral zone (the range of core body temperatures your brain considers normal) means even a slight rise triggers a full vasomotor response: blood vessels dilate, skin flushes, heart rate increases, and sweating begins.
This process involves neurokinin B (NKB) signaling in the hypothalamus. When estrogen is present, it helps regulate NKB activity. Without sufficient estrogen, NKB neurons fire more aggressively, triggering hot flashes that can last from a few seconds to several minutes. The National Institute on Aging notes that hot flashes typically last 5 to 7 years but can persist for 15 years or more in some women.
Sleep disruption during menopause has a similar hormonal root. Declining estradiol and rising FSH levels alter melatonin secretion and circadian rhythm regulation. Research from a scoping review published in Life found that about 30% of pre-menopausal women report sleep problems, a figure that climbs to 50% in postmenopausal women. The multiethnic SWAN study tracked menopausal women for 10 years and found that 46 to 48% experienced insomnia, compared with 38% of premenopausal women.
Night sweats add another layer: even when a hot flash doesn't fully wake you, the brain changes preceding the flash can disrupt sleep architecture. Johns Hopkins Medicine explains that research shows many menopausal women actually awaken just before a hot flash occurs, suggesting the neurological trigger itself interrupts sleep, not just the heat sensation. Postmenopausal women are also two to three times more likely to develop sleep apnea compared with premenopausal women.
Phytoestrogens: What the Research Actually Shows
Phytoestrogens are plant compounds structurally similar to human estrogen. They bind to estrogen receptors, though much more weakly than actual estrogen. The three main types relevant to menopause are isoflavones (found in soy and red clover), lignans (found in flaxseed), and coumestans (found in alfalfa and clover sprouts).
Quick fact: Over 300 plants with phytoestrogen components have been identified, but only a handful have been studied in clinical trials for menopausal symptoms.
Soy isoflavones
Soy has the most research behind it. Pooled data from clinical trials shows that soy isoflavone supplements at a median dose of 54 mg aglycone equivalents reduced hot flash frequency by about 20.6% and severity by 26.6%. Those numbers are real, but they're modest. The NCCIH notes that the overall evidence doesn't consistently support soy products for menopausal symptom relief, partly because study quality varies widely.
One reason Asian women report fewer menopausal symptoms may be lifelong dietary exposure to soy. Starting soy supplements at age 50 is different from consuming tofu and edamame since childhood. The gut microbiome's ability to convert isoflavones into equol (the active metabolite) varies between individuals, with only about 30 to 50% of Western women producing equol efficiently.
Red clover
Red clover contains isoflavones similar to soy, particularly biochanin A and formononetin. Some trials suggest modest benefits for hot flash reduction, but systematic reviews have found the evidence inconsistent. Red clover may offer mild antioxidant and cardiovascular protection, though these effects need more study.
Flaxseed
Flaxseed is rich in lignans and omega-3 fatty acids. The evidence for hot flash reduction is weak. Controlled trials show little difference between flaxseed supplementation and placebo for vasomotor symptoms, though flaxseed may benefit cardiovascular health through other mechanisms.
| Phytoestrogen | Source | Hot Flash Reduction | Evidence Quality |
|---|---|---|---|
| Soy isoflavones | Tofu, edamame, supplements | ~20% frequency, ~27% severity | Moderate (mixed results) |
| Red clover | Supplements (Promensil) | Small to none | Low (inconsistent) |
| Flaxseed lignans | Ground flaxseed, flax oil | Minimal | Low (not superior to placebo) |
Black Cohosh and Other Herbal Approaches
Black cohosh (Cimicifuga racemosa) is probably the most widely used herbal supplement for menopause symptoms in the United States. Despite decades of research, the evidence is still mixed.
A 2023 meta-analysis published in Menopause found that black cohosh extracts were associated with significant improvements in overall menopausal symptoms, hot flashes, and somatic symptoms compared with placebo. However, it did not significantly improve anxiety or depressive symptoms. One wrinkle: black cohosh works through serotonergic pathways, not estrogenic ones. It should not be classified as a phytoestrogen despite common marketing claims.
The most-studied formulation is the isopropanolic extract (sold as Remifemin). A 2020 review and meta-analysis in Climacteric found that this specific extract showed consistent benefits across multiple trials. Generic "black cohosh" supplements may not deliver the same results because extraction methods and plant part ratios vary considerably between manufacturers.

Other herbs with some evidence
| Herb | Mechanism | Evidence for Menopause | Safety Notes |
|---|---|---|---|
| Valerian | Increases GABA in synaptic cleft | Moderate for sleep; mixed for hot flashes | Generally safe short-term |
| Sage (Salvia officinalis) | Binds GABA/benzodiazepine receptors; phytoestrogenic | Promising for sweats and hot flashes | Avoid high doses long-term |
| Passionflower | GABA-A receptor activation | Limited but positive for sleep | Generally safe |
| St. John's Wort | Benzodiazepine receptor activation | Some benefit for mood; limited for hot flashes | Major drug interactions (SSRIs, oral contraceptives) |
| Vitex (Chasteberry) | Progesterone receptor expression | Some evidence for hot flashes | May interact with hormonal medications |
The Electron Physician review documented clinical trial evidence for each of these herbs, noting that while many show some benefit, most studies are small and short-term. No herbal remedy consistently outperforms placebo by the same margin that hormone therapy does. If you're interested in herbal approaches for stress management alongside menopause symptoms, ashwagandha is another adaptogen worth researching, though its evidence for hot flashes specifically is limited.
Mind-Body Practices That Measurably Reduce Symptoms
If the supplement section left you underwhelmed, fair enough. The numbers for mind-body interventions are a different story. Several of these approaches have held up across multiple rigorous trials, and the effect sizes actually compete with medication.
Hypnotherapy
This one surprises people. In a randomized clinical trial of 187 women, hypnosis reduced subjective hot flash frequency by 74% and hot flash interference by 80%. Physiologically monitored hot flashes (not self-reported, but measured with skin conductance monitors) dropped by 57%. Those numbers rival medication. The North American Menopause Society now recommends hypnosis for hot flash management based on this evidence.
In a pilot study, hypnosis alone matched venlafaxine 75 mg (an SSRI commonly prescribed off-label for hot flashes), both cutting hot flash severity scores by 50%. The placebo group saw 25%. Five sessions with a trained hypnotherapist is the typical protocol, so it's not a massive time commitment.
Cognitive behavioral therapy (CBT)
CBT addresses both hot flash distress and insomnia. For hot flashes specifically, a 6-week CBT program reduced hot flash interference by 52% in breast cancer survivors. For insomnia, CBT-I (the insomnia-specific protocol) is even more impressive.
A MsFLASH randomized clinical trial testing telephone-delivered CBT-I found that at 8 weeks, 70% of women in the CBT-I group achieved no insomnia compared with just 24% in the control group. At 24 weeks, those numbers were 84% versus 43%. A 2015 meta-analysis of 20 RCTs showed CBT-I reduced sleep latency by an average of 19 minutes and wake-after-sleep-onset by 26 minutes, while improving sleep efficiency by 10%.
CBT-I works differently from sleep medication. Instead of sedating you, it retrains how your brain handles sleep through sleep restriction, stimulus control, and cognitive restructuring. The benefits stick around after treatment ends because you've changed the underlying patterns.
If you're dealing with stress-related sleep problems beyond menopause, understanding how chronic stress affects your hormonal axis can help you address the full picture.
Yoga and meditation
The evidence for yoga is more modest. Several trials show yoga may reduce the perceived bothersomeness of hot flashes and improve sleep quality, though it doesn't consistently reduce hot flash frequency. Mindfulness meditation shows similar patterns: better stress coping and improved quality of life measures, but limited direct impact on vasomotor symptoms. Still, both practices contribute to the kind of nervous system regulation that supports better overall sleep.
Supplements for Sleep During Menopause
Sleep trouble during menopause doesn't always track with hot flash severity. Some women sleep poorly even when hot flashes are mild, because the underlying hormonal changes mess with sleep architecture on their own.
Melatonin
Melatonin production naturally declines with age, and the menopausal hormonal shift compounds this. Research shows that melatonin at doses of 3 mg or more can improve both sleep quality and, surprisingly, hot flashes and night sweats in menopausal women. However, there's a significant quality control problem: studies have found that actual melatonin content in supplements varies from 83% less to 478% more than what labels claim.
For menopausal sleep specifically, low-dose melatonin (0.5 to 3 mg) taken 30 to 60 minutes before bed appears most effective. Higher doses aren't necessarily better and can cause morning grogginess.
Magnesium
Magnesium plays a role in GABA receptor function, the same neurotransmitter system that many sleep medications target. While there aren't many trials specifically in menopausal women, magnesium supplementation has shown benefits for sleep quality in older adults generally. The systematic review in Nutrition Reviews included magnesium among nutritional interventions that showed benefit for menopause-related sleep disturbances. Magnesium glycinate and magnesium threonate are the forms most commonly recommended for sleep support. For a deeper look at choosing between forms, see our guide on magnesium types.
Valerian
Valerian root increases GABA availability in the brain. General insomnia research calls it unreliable, but it may work better specifically for perimenopausal women. Clinical trials in this population show improvements in sleep quality, sometimes immediate and more significant after 4 weeks of consistent use. Combined valerian and fennel preparations have shown benefits for both hot flashes and sleep quality in multiple randomized trials.
Other options
| Supplement | Typical Dose | Evidence Level | Notes |
|---|---|---|---|
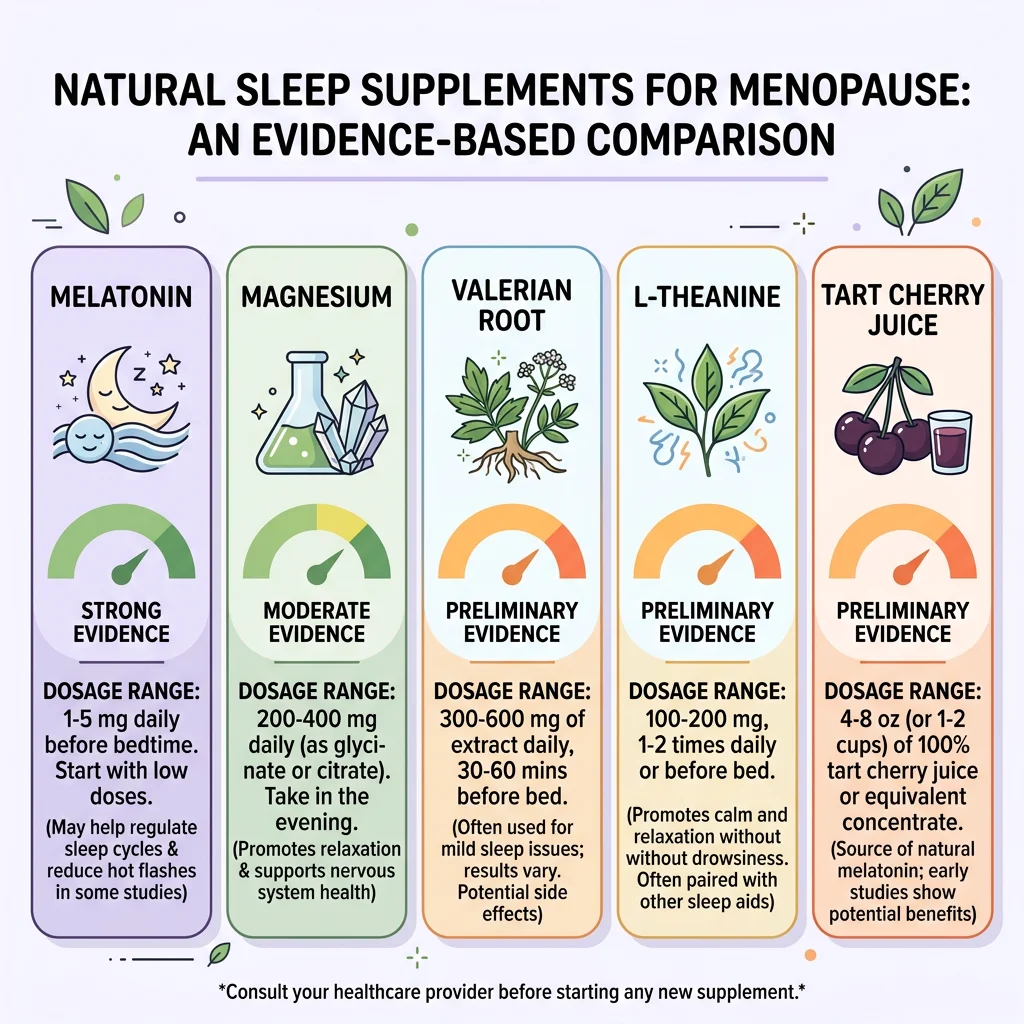
| Melatonin | 0.5-3 mg before bed | Moderate | Quality control varies widely between brands |
| Magnesium glycinate | 200-400 mg before bed | Moderate (general sleep) | Low risk of side effects |
| Valerian root | 300-600 mg before bed | Moderate (perimenopausal) | Allow 2-4 weeks for full effect |
| L-theanine | 200 mg before bed | Preliminary | Promotes relaxation without sedation |
| Tart cherry juice | 240 ml twice daily | Preliminary | Natural melatonin source; may reduce inflammation |
If you're curious about tart cherry juice specifically, we've covered the research on tart cherry for sleep and recovery in detail.
Free Lifestyle Fixes Worth Trying First
Before spending money on supplements, a few no-cost changes have surprisingly solid evidence behind them.
Keep your bedroom cold
Aim for 60 to 67 degrees Fahrenheit. Use layered, breathable bedding (cotton or bamboo) you can kick off quickly. A cooling pillow or mattress pad can reduce nighttime awakening from hot flashes. The NIA recommends drinking small amounts of cold water before bed and keeping a fan within reach.
Exercise, but time it right
Regular exercise helps menopausal women both fall asleep and stay asleep. Johns Hopkins notes that even non-athletes see improved sleep efficiency with consistent movement. The catch: avoid vigorous exercise within 3 hours of bedtime. It raises core body temperature and can trigger the exact hot flashes you're trying to prevent.
Watch the afternoon coffee (and the wine)
Alcohol, caffeine, and spicy foods are well-documented hot flash triggers. Caffeine has a half-life of 5 to 6 hours, so that 2 p.m. latte is still half-active in your system at 8 p.m. Alcohol is worse in a subtler way: it may help you fall asleep initially but fragments sleep architecture in the second half of the night, right when night sweats tend to peak.
Sleep hygiene specifics for menopause:
- Keep a consistent sleep and wake schedule, even on weekends
- Limit screen exposure for at least one hour before bed
- Wear moisture-wicking sleepwear (cotton or technical fabrics)
- Use the bed only for sleep and intimacy, not reading or watching television
- If a hot flash wakes you and you can't fall back asleep within 20 minutes, get up and do something calm in dim light until sleepiness returns
Weight and hot flash frequency
The NIA notes that women who are overweight or obese experience more frequent and severe hot flashes. Even modest weight loss, around 5 to 10% of body weight, can reduce how often they happen. Understanding how circadian rhythms affect sleep quality can also help you time these lifestyle changes for better results.
What Doesn't Work: Myth vs. Evidence
Some of the most popular menopause remedies have almost no clinical support. Worth knowing before you spend the money.
| Claim | Reality | Verdict |
|---|---|---|
| "DHEA eliminates hot flashes" | The NIA specifically lists DHEA as unproven for hot flashes. Limited evidence, potential hormonal side effects. | Not supported |
| "Evening primrose oil cures menopause symptoms" | Minimal clinical evidence. Contains gamma-linolenic acid but trials show little benefit for vasomotor symptoms. | Not supported |
| "Any black cohosh supplement works the same" | Extraction method matters significantly. Only the isopropanolic extract (Remifemin) has consistent positive trial data. | Partially true (formulation-dependent) |
| "Soy foods eliminate hot flashes" | Modest benefit (~20% reduction). Individual response varies based on gut bacteria's ability to produce equol. | Modest benefit, not elimination |
| "Bioidentical hormones are risk-free" | Compounded bioidentical hormones carry similar risks to conventional hormone therapy. FDA-approved bioidentical options exist with established safety data. | Misleading marketing |
| "Acupuncture reliably reduces hot flashes" | Some studies show benefit, but systematic reviews find results inconsistent and often not superior to sham acupuncture. | Inconclusive |

Frequently Asked Questions
What is the single most effective natural remedy for hot flashes?
Based on clinical trial data, clinical hypnosis has the strongest evidence among non-hormonal, non-pharmacological approaches. A randomized trial of 187 women found hypnosis reduced hot flash frequency by 74% and interference by 80%. Five sessions with a trained hypnotherapist is the standard protocol. The North American Menopause Society recommends hypnosis for hot flash management.
Can I take black cohosh long-term?
Most clinical trials have studied black cohosh for 6 months or less. The NCCIH notes that while short-term use appears generally safe, there have been rare reports of liver damage associated with black cohosh products. If you choose to use it, stick with a standardized extract (the isopropanolic formulation has the most safety data), and discuss it with your healthcare provider, especially if you have liver conditions or take medications processed by the liver.
Does melatonin help with menopause hot flashes or just sleep?
Both, potentially. Research shows melatonin at 3 mg or higher can improve hot flashes and night sweats in addition to sleep quality. However, supplement quality varies enormously, so choose a brand that has been third-party tested (look for USP or NSF certification on the label).
How long does CBT-I take to work for menopause-related insomnia?
Most CBT-I protocols run 4 to 6 sessions over 6 to 8 weeks. In the MsFLASH trial, 70% of women in the CBT-I group had no insomnia after 8 weeks, and improvements continued at 24 weeks (84% with no insomnia). Unlike sleep medication, CBT-I benefits persist after treatment ends because you've retrained your sleep patterns rather than relying on a chemical intervention.
Are phytoestrogens safe for women with a history of breast cancer?
This is a question for your oncologist, not a supplement label. The long-term safety of phytoestrogens in women with estrogen-receptor-positive breast cancer has not been established. The NCCIH states that the long-term safety of phytoestrogens such as soy, red clover, and flaxseed has not been established in this population. Some oncologists permit dietary soy (tofu, edamame) in moderate amounts but advise against concentrated isoflavone supplements.
Related Articles
- Ashwagandha Benefits, Dosage, and Side Effects - A detailed look at this adaptogen's evidence for stress, sleep, and hormonal balance.
- Magnesium Types: Glycinate, Citrate, and Threonate Compared - Which form of magnesium is best for sleep, anxiety, and muscle recovery.
- Best Ways to Improve Your Sleep - Practical strategies for better sleep quality backed by research.
- Chronic Stress, Hormones, and HPA Axis Recovery - How prolonged stress disrupts your hormonal system and what helps restore balance.
- Tart Cherry Juice for Sleep, Recovery, and Inflammation - The research behind this natural melatonin source.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.









